
SPNS Supporting Replication (SURE) of Housing Interventions Request For Proposal (RFP)
A Request for Proposal (RFP) is now available to Ryan White HIV/AIDS Program (RWHAP) service providers for a Special Project of National Significance (SPNS) program titled Supporting Replication (SURE) of Housing Interventions. It includes funding for up to 10 implementation sites that will implement and adapt housing-related intervention strategies for three priority populations of people with HIV experiencing unstable housing.
The purpose of the SURE Housing initiative is to implement and adapt housing-related intervention strategies for three priority populations of people with HIV experiencing unstable housing, who often have the highest HIV-related disparities:
1) people who identify as lesbian, gay, bisexual, transgender, and queer or questioning (LGBTQ+);
2) youth and young adults (aged 18-24); and
3) people who have been justice-involved (defined as any person who is engaged at any point along the continuum of the criminal justice system as a defendant including arrest, incarceration, and community supervision).
The goal of this initiative is to promote the replication of effective housing interventions in the RWHAP to decrease health and housing disparities and improve health outcomes along the HIV care continuum. This initiative will engage and retain people with HIV experiencing unstable housing in HIV medical care and support services by addressing their housing and behavioral health needs, as needed.
Serving as the Implementation and Technical Assistance Provider, the Corporation for Supportive Housing (CSH), in partnership with Collaborative Solutions, Inc (CSI), will select, issue, and monitor sub-awards of up to $250,000 per funding year for up to ten implementation sites. Sites will be funded from May 1, 2023 – July 31, 2026. CSH and CSI will provide the sites with technical assistance (TA) for implementing and adapting these interventions.
The implementation sites will also participate in a multi-site evaluation to assess the effectiveness of the interventions’ implementation and adaptation. The implementation of housing-related interventions at each site will be evaluated by the Evaluation Provider comprised of Boston University, the University of Massachusetts, Lowell, and JSI Research & Training Institute, Inc.
Additional information can be found in the Request for Proposals.
Application Details
Current RWHAP service providers are eligible to apply. Applications are due no later than 11:59pm ET on February 15, 2023. To learn more about this opportunity, register here for a live webinar taking place on January 10, 2023 at 3PM Eastern.
For more information, contact HRSA.TA@CSH.ORG.

 More than 160,000 Americans are unaware they are living with HIV. Diagnosing HIV is critical to the success of the Ending the HIV Epidemic in America initiative (EHE). How can we assist clinical providers in identifying individuals who would not otherwise receive HIV testing? Research demonstrates large-scale HIV screening in the emergency departments and urgent care settings using existing staff and resources, regardless of patient selection strategy, does not impact care processes or patient flow.
More than 160,000 Americans are unaware they are living with HIV. Diagnosing HIV is critical to the success of the Ending the HIV Epidemic in America initiative (EHE). How can we assist clinical providers in identifying individuals who would not otherwise receive HIV testing? Research demonstrates large-scale HIV screening in the emergency departments and urgent care settings using existing staff and resources, regardless of patient selection strategy, does not impact care processes or patient flow.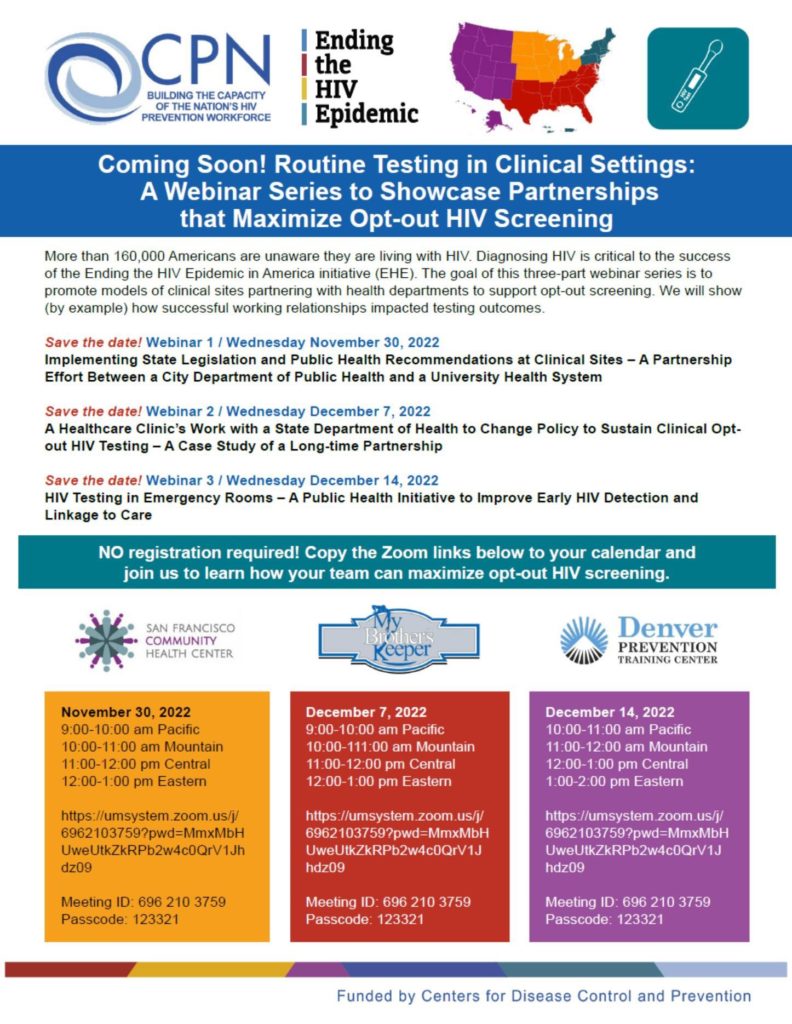
 Starting antiretroviral treatment (ART) early in the course of HIV infection when the immune system is stronger results in better long-term health outcomes compared with delaying ART, according to findings presented at the IDWeek Conference in Washington, D.C.
Starting antiretroviral treatment (ART) early in the course of HIV infection when the immune system is stronger results in better long-term health outcomes compared with delaying ART, according to findings presented at the IDWeek Conference in Washington, D.C.