Cross-posted from HIV.gov
New CDC MMWR Articles: Increasing Equity in Monkeypox Vaccine Distribution
Last Friday, CDC published three new Morbidity and Mortality Weekly Report (MMWR) reports on recent developments in monkeypox vaccination in the U.S.:
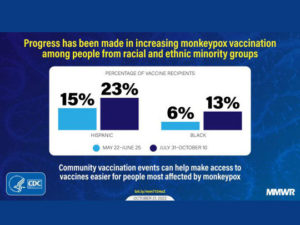
The first report shows that progress has been made in increasing the proportion of Black and Hispanic persons vaccinated against monkeypox virus in the U.S. According to the report, by October 10, 2022, 931,155 JYNNEOS vaccine doses were administered in the United States. Among persons who received ≥1 vaccine dose, 51.4% were non-Hispanic White, 12.6% were non-Hispanic Black or African American (Black), and 22.5% were Hispanic persons. The percentages of vaccine recipients who were Black (5.6%) and Hispanic (15.5%) during May 22–June 25 increased to 13.3% and 22.7%, respectively, during July 31–October 10. The Importance of Community Vaccination Events The other reports detail how community vaccination events can help make access to vaccines easier for people most affected by monkeypox. This summer’s Southern Decadence event in Louisiana and the Atlanta Black Gay Pride Festival in Georgia are highlighted. Both events provided the opportunity to increase access to monkeypox vaccination among populations disproportionally affected by the monkeypox outbreak. Community engagement, targeted messaging, and selection of venues catering primarily to racial and ethnic minorities for community vaccination events improved vaccine equity and reduced health disparities. For the latest information on monkeypox in the U.S., visit CDC.gov.
Addressing Monkeypox Holistically
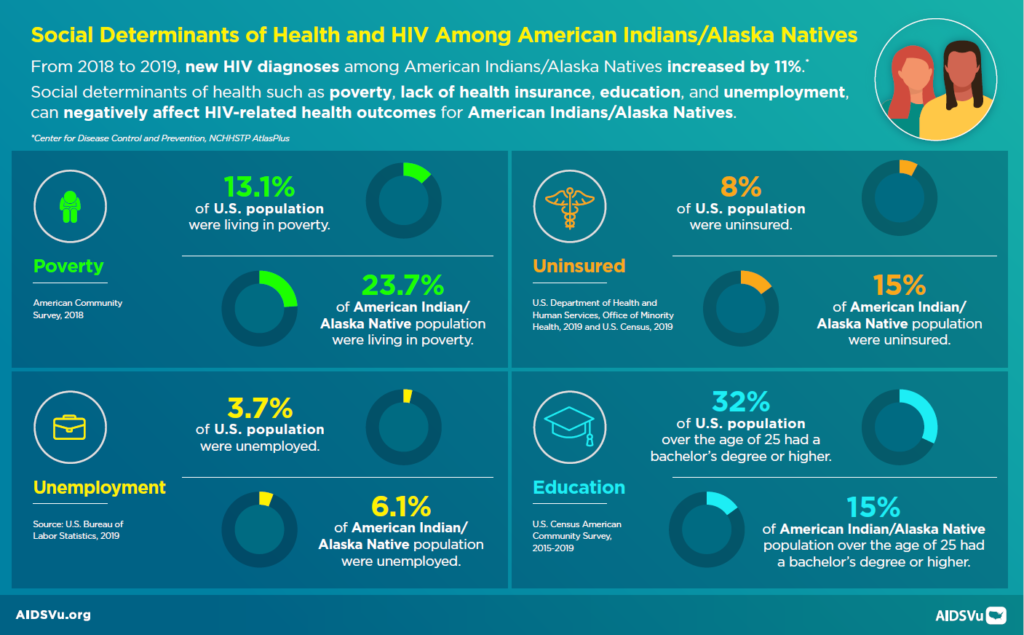
 From day one of the Biden Administration’s response to the Monkeypox outbreak, we have recognized that Monkeypox is not a virus that lives in isolation. It exists as a part of a number of acute and chronic outbreaks and health challenges that interact with each other and can be impacted by social circumstances that worsen disease outcomes. Such interacting epidemics, or “syndemics,” require responses beyond traditional disease-specific healthcare delivery and to also address associated social determinants of health. That’s why we have worked closely—and successfully—within the Administration and with our partners in public health, the LGBTQI+ community, and with community-based organizations—to combat and treat this virus using a holistic approach, that takes all of these factors into consideration.
From day one of the Biden Administration’s response to the Monkeypox outbreak, we have recognized that Monkeypox is not a virus that lives in isolation. It exists as a part of a number of acute and chronic outbreaks and health challenges that interact with each other and can be impacted by social circumstances that worsen disease outcomes. Such interacting epidemics, or “syndemics,” require responses beyond traditional disease-specific healthcare delivery and to also address associated social determinants of health. That’s why we have worked closely—and successfully—within the Administration and with our partners in public health, the LGBTQI+ community, and with community-based organizations—to combat and treat this virus using a holistic approach, that takes all of these factors into consideration.
HIV and Monkeypox are examples of syndemic outbreaks that interact with each other and therefore require specific action for both diseases in order to mitigate the impact of both. Recent epidemiology has shown that people with HIV continue to be over-represented in cases and severe manifestations of Monkeypox disease. In one study published by the CDC, nearly 40% of people diagnosed with Monkeypox had HIV infection, and over 40% had been diagnosed with a sexually transmitted infection (STI) in the year prior to their Monkeypox diagnosis.1
In an even more recent study of 57 people reported to CDC with severe Monkeypox infections, 82% had advanced HIV infection and nearly three-quarters of these individuals had very compromised immune systems with extremely low CD4 cell counts. Under 9% of these patients were taking antiretrovirals at the time of their Monkeypox diagnosis. Some people succumbed to these preventable infections.2
Syndemics are not just about viruses and bacteria; social circumstances like systemic inequities in the health care system and social determinants of health like housing interact with infections to worsen or deepen their impact. In this same report of severe Monkeypox outcomes, nearly 70% of patients were Black and 23% were experiencing homelessness.2
These statistics make it clear the need to continue an aggressive and comprehensive approach to address Monkeypox, HIV, STIs, homelessness, and mental health together. HIV prevention and care mitigates the impact of Monkeypox on the health of individuals living with or at-risk for both infections. And, linkage to HIV care and treatment is critical to protect individuals from a variety of health threats, including Monkeypox.
Throughout our response to the Monkeypox outbreak, the Biden-Harris Administration has taken critical actions toward this effort. We have centered vaccine equity with local and national programs to address disparities in vaccine administration by bringing vaccine closer to the people who could benefit. HRSA’s Ryan White HIV/AIDS Program, CDC, SAMSHA, and HUD have worked with grantees to emphasize the urgent need for syndemic actions to respond to syndemic challenges. These agencies have provided clear messages about the importance of using the HIV, STIs, housing, and behavioral health funding, staff, and infrastructure to help control Monkeypox. It is critical that front line service providers in public health departments, medical clinics, substance abuse and mental health environments, housing providers, and community-based organizations continue to leverage these resources across these syndemics. We can work collaboratively across these interacting infections and social determinants to address the Monkeypox virus as a holistic health challenge, not in isolation. Providers that serve affected communities, particularly those living with HIV, must continue to leverage funding and programmatic flexibilities by:
- Using HIV care systems to support people with HIV and lead those at-risk for Monkeypox to the testing, prevention, and treatment services required to prevent poor outcomes of both diseases.
- Using established data-to-care strategies, and out-of-care lists, to reach the people most vulnerable for severe illness because they are not engaged in HIV care and use that outreach to offer them Monkeypox vaccine, behavioral guidance, and linkage to HIV care.
- Taking the opportunity presented by people seeking Monkeypox prevention to test for HIV and STIs and offer prevention or treatment services to avoid HIV infection or disease progression.
- Using housing resources to support people living with HIV and others so that they can prioritize their Monkeypox and HIV-related health seeking behaviors.
- Taking advantage of housing and mental health service encounters to engage people with HIV at-risk for Monkeypox and to link them with resources to identify, prevent, or mitigate Monkeypox and HIV disease progression.
- Provide HIV and Monkeypox resources and services for people seeking STI diagnosis and treatment.
Because Monkeypox exists as part of the syndemic of HIV, STIs, mental health and homelessness, the Administration is committed to treating it that way. Providers must continue to use all of the tools created by these important, and ground-breaking, funding and programmatic flexibilities. Service providers should use the expanded syndemic toolkit created by these flexibilities including HIV data-to-care, care navigation, housing resources, HIV prevention and care services, and Monkeypox vaccine and education to control this outbreak and support the wellness of people with and at-risk for HIV.
Resources
Learn More About Monkeypox: HHS Response to the Monkeypox Outbreak | HHS.gov
Ryan White Monkeypox Resources: Monkeypox Information | Ryan White HIV/AIDS Program (hrsa.gov)
Prevent Monkeypox: Prevention | Monkeypox | Poxvirus | CDC
Mental Health and Monkeypox: Monkeypox (MPV) | SAMHSA
HUD Monkeypox Resources: and
References
- Curran KG, Eberly K, Russell OO, et al. HIV and Sexually Transmitted Infections Among Persons with Monkeypox — Eight U.S. Jurisdictions, May 17–July 22, 2022. MMWR Morb Mortal Wkly Rep 2022;71:1141–1147. DOI: http://dx.doi.org/10.15585/mmwr.mm7136a1
- Miller MJ, Cash-Goldwasser S, Marx GE, et al. Severe Monkeypox in Hospitalized Patients — United States, August 10–October 10, 2022. MMWR Morb Mortal Wkly Rep. ePub: 26 October 2022. DOI: http://dx.doi.org/10.15585/mmwr.mm7144e1
 More than 160,000 Americans are unaware they are living with HIV. Diagnosing HIV is critical to the success of the Ending the HIV Epidemic in America initiative (EHE). How can we assist clinical providers in identifying individuals who would not otherwise receive HIV testing? Research demonstrates large-scale HIV screening in the emergency departments and urgent care settings using existing staff and resources, regardless of patient selection strategy, does not impact care processes or patient flow.
More than 160,000 Americans are unaware they are living with HIV. Diagnosing HIV is critical to the success of the Ending the HIV Epidemic in America initiative (EHE). How can we assist clinical providers in identifying individuals who would not otherwise receive HIV testing? Research demonstrates large-scale HIV screening in the emergency departments and urgent care settings using existing staff and resources, regardless of patient selection strategy, does not impact care processes or patient flow.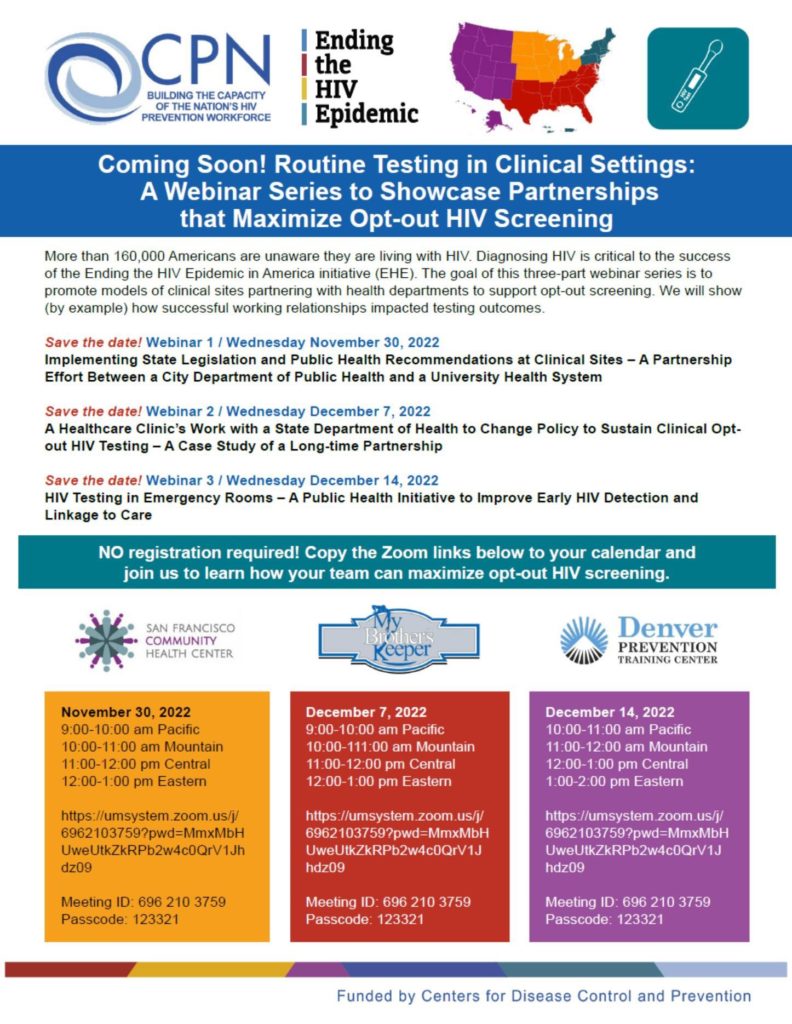
 Starting antiretroviral treatment (ART) early in the course of HIV infection when the immune system is stronger results in better long-term health outcomes compared with delaying ART, according to findings presented at the IDWeek Conference in Washington, D.C.
Starting antiretroviral treatment (ART) early in the course of HIV infection when the immune system is stronger results in better long-term health outcomes compared with delaying ART, according to findings presented at the IDWeek Conference in Washington, D.C.