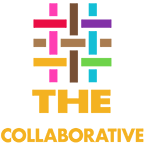
Behavioral and Clinical Characteristics of Persons with Diagnosed HIV Infection—Medical Monitoring Project, United States 2020 Cycle (June 2020–May 2021)
This new report finds that services like dental care, housing, and SNAP/WIC can help people with HIV access and stay in routine HIV care and be virally suppressed, but those needs are not always met.
The HIV Clinical Leadership Program is an established, postdoctoral fellowship aimed at developing HIV specialists who are knowledgeable and committed to addressing the health inequities our patients face at an individual and systemic level. The HIV Clinical Leadership Program have a proven track record of placing fellows in competitive leadership career positions throughout the United States.
Candidates will be competitively selected through a national search for this two-year clinical fellowship program. Those selected will participate in the HIV Clinical Leadership Program with full fellowship salary and benefits.
Up to 4 fellows may be selected for each cohort.
Fellows with eligible academic loans may receive up to $150,000 in loan repayment if they continue to provide HIV-related services in undeserved communities.
Desired qualifications for potential candidates include:
A strong interest in primary care and HIV medicine
A strong interest in pursuing and implementing outpatient quality improvement or system innovation
A sincere commitment to work with underserved communities
Due to the current trends of the HIV epidemic in the United States, physicians from the South and Mid-Atlantic states strongly encouraged to apply!
Black, Latinx, Indigenous, BIPOC, LGBTQIA2S+ physicians strongly encouraged to apply!
Consumer fact sheets on HIV and Pregnancy are available from HIVinfo. Fact sheets from HIVinfo provide important information about ways to prevent perinatal transmission of HIV (transmission from mother to child).
Each fact sheet includes a summary of key points and links to additional information and resources.
View the fact sheets:
Visit the Understanding HIV section of the HIVinfo website to browse the complete collection of HIVinfo’s consumer education materials, including fact sheets, infographics, and an HIV glossary.
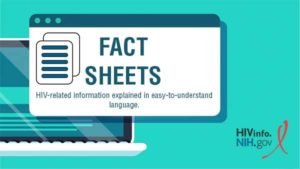
As the 2022 monkeypox outbreak accelerates, the U.S. Centers for Disease Control and Prevention released a Dear Colleague Letter for healthcare providers and care team members highlighting the importance of addressing pain control in people with monkeypox.